|
||||||||
| LEAD Action News Volume
12 Number 4, June 2012, ISSN 1324-6011 Incorporating Lead Aware Times ( ISSN 1440-4966) and Lead Advisory Service News (ISSN 1440-0561) The Journal of The LEAD (Lead Education and Abatement Design) Group Inc. Joint Editors: Elizabeth O’Brien and Anne Roberts |
||||||||
|
About Us
|
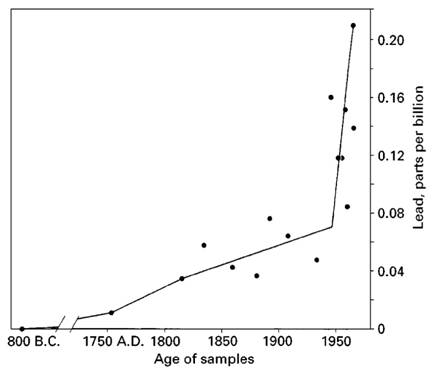
Eliminating Childhood Lead Toxicity in Australia: A Little is Still Too Much. Macquarie University Lead Forum 5th July 2012. Chris Winder, PhD, Professor of OHSE Management, Faculty of Business, Australian Catholic University, North Sydney NSW 2060 Keywords: Lead, toxicity of lead, lead exposure, pediatric lead effects, adult lead effects, environmental lead, lead risk, level of concern Background The experience of people in the modern world with lead is one of poorly considered impacts, extensive and poorly controlled exposures, and poorly characterised environmental and human impacts.[i],[ii],[iii] Over one hundred years ago, in 1904, the Scottish born Australian physician J Lockhart Gibson was among the first English-language authors to directly link lead-based paint to childhood lead poisoning, specifically noting the dangers to children from painted walls and verandas of houses in Queensland.[iv] In 1909, another physician working in Australia, Dr Alfred Jefferis Turner, was the first to suggest that preventive approaches that identify, and then remove exposures to lead offered the most effective way to protect children from the effects of lead.[v] Environmental Accumulation of Lead Throughout the twentieth Century, exposures increased, but the views of public health and environmental professionals (including Gibson and Turner) that lead was damaging the health of adults, but more particularly children, were largely ignored. In 1969, work by Clare Patterson and colleagues suggested that environmental lead levels had increased since Roman times, increasing gradually from the start of the industrial revolution, and increasing exponentially since the introduction of lead in petrol (until at least the 1970s). Figure 1 shows data from analysis of snow cores from Greenland. Figure 1: Lead Contamination of Greenland Snow Cores
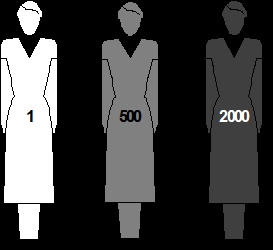
From this, Patterson suggested current lead loads in humans, while not necessarily dangerous, were in fact orders of magnitude higher than our prehistoric ancestors.vi Figure 2, presents the view that modern day human lead burdens were already sufficiently high to suggest the margin of safety from “normal” to toxic levels was very small. Figure 2: Comparison of Relative Amounts of Lead in People
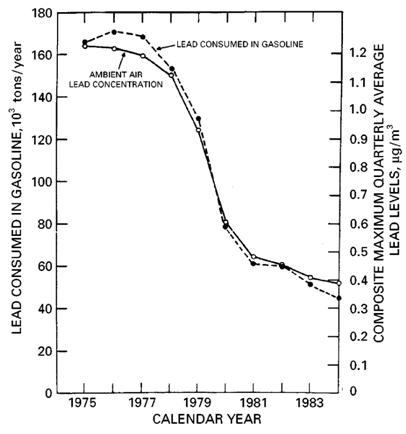
Modern humans had body lead loads hundreds of times higher than their forebears, perhaps showing subclinical toxic effects across an entire population. The USA moved to remove lead from petrol in 1972. Lead levels in air fell from 1.2 µg/m3 in 1975 to 0.4 µg/m3 in 1984, following closely the fall in consumption of lead in petrol (see Figure 3 below). Figure 3: Relationship between Lead in Petrol Consumption and Lead in Air
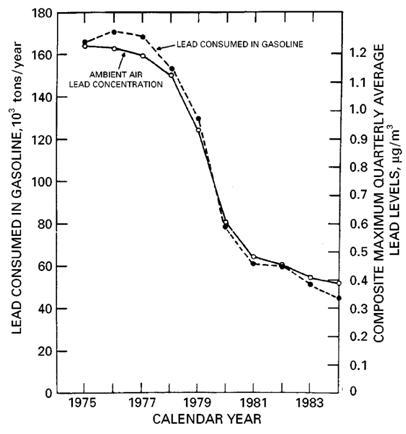
Further, the decrease was mirrored by a decline in population blood leads from about 16 µg/dL in 1976, to below 10 µg/dL in 1980 (see Figure 4 below). Figure 4: Relationship between Lead in Petrol Consumption and Lead in Blood
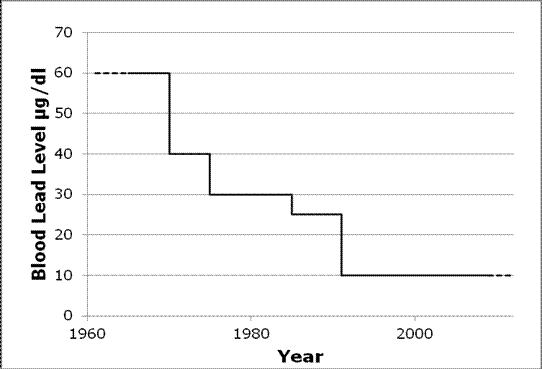
Population blood levels continued to fall in the USA. By 1990, median US population blood levels were down to 2.8 µg/dL.[viii] Leaded petrol marketed by the Commonwealth Oil Refineries was being sold in Australia from at least August 1932.[ix] In 1985, changes to Australian Design Rules for catalytic converters to be included in motor vehicles were introduced. Lead free petrol was available from then, but the availability of leaded petrol continued to 2002. Development of the Pediatric “Level of Concern” As evidence increased from multiple studies showing loss of mental capacity in children, even when no pathology was observed, the concept of a “level of concern” for lead exposure in poisoned children emerged. This level was one that pediatricians could use for establishing priorities and interventions for the lead poisoned child. In about 1960, Health agencies in Europe and the USA set, and then lowered, this level of concern from 60 μg/dL, to 40 μg/dL (in 1971), to 30 μg/dL in 1985, and lastly, to 10 μg/dL in 1991 (see Figure 5).[x],[xi],[xii] Figure 5: Changes to the Blood Lead Level of Concern in the USA
In 1979, a breakthrough study by Herb Needleman and colleagues related lead in children’s teeth to diminished mental capacity.[xiii] Epidemiological evidence demonstrating adverse effects of lead on children’s neurodevelopment, including reduced IQ scores and learning difficulties, at lower and lower exposures accumulated throughout the 1970s, 1980s and 1990s. In 1992, at an International Conference held in Melbourne, discussions around the nature of the level of concern and its move from a blood lead number that related to a pediatric emergency, to considerations emerged that a means of managing a public health risk was needed.[xiv] At the time, one of the reasons that 10 μg/dL was retained as a criterion for lead exposure, was not because it was a safe level, or even because it was the upper limit of normal, but because it was recognised that the psychological tools available at the time were too crude to measure functional neuropsychological deficits in young children with any degree of accuracy. Notwithstanding these difficulties, agencies such as the US CDC[xv] and the NHMRC[xvi] continued to issue guidance to health professionals about what should be done when confronted with a child with elevated lead exposure. These agencies suggested that a blood level of 10 µg/dL should be used as a level above which levels are regarded as elevated, and that investigation or intervention is recommended. What should now be done? That was over twenty years ago. Since then, more and more studies have shown that blood lead levels below 10 μg/dL harm children.[xvii] Furthermore, these affects are not just seen in intelligence, but also cardiovascular, immunological and endocrine effects. Additionally, at least some of these impacts are irreversible. It also appears that such effects do not appear to be confined to children of lower socioeconomic status. What perhaps is less well known is that evidence is also emerging to indicate that lead may also be affecting the cardiovascular, renal, reproductive health and cognitive function of adults at levels lower than previously considered, and in some cases below 10 μg/dl.[xviii] Some of these findings support the possible persistence of lead induced effects in childhood into adulthood.[xix],[xx] So, the idea of a “level of concern” is becoming obsolete, except for action in clinical cases. In 2010, the German Federal Environment Agency moved to the term “reference value” and set its value based on the 95th percentile of blood lead levels from national blood lead surveys as their new trigger levels for action,[xxi] arriving at:
In the US, in November 2011, the National Toxicology Program published a draft monograph on Health Effects of Low Level Lead,[xxii] which reported that “there is sufficient evidence for adverse health effects in children and adults at blood Pb [lead] levels below 10 μg/dL [micrograms per deciliter] and below 5 μg/dL as well.” These health effects included adverse associations for cardiovascular, renal and immune health outcomes. In January 2012, a report of the CDC Advisory Committee on Childhood Lead Poisoning Prevention (ACCLPP), made a recommendation (subsequently accepted by the US CDC), that the term “level of concern” be eliminated.[xxii] The ACCLPP also recommended that a reference value of 5 μg/dL be used to identify children who have an elevated blood lead level, based on the 97.5 percentile for children aged 1-5.[xxii] This level should trigger lead education, parental advice on nutrition, environmental investigations, and if warranted, additional health surveillance. In Australia, the NHMRC are investigating this issue. The focus now should be on identifying sources, assessing risks and eliminating exposures, with the fundamental aim of primary prevention as now noted by such agencies as the World Health Organisation (WHO) and US CDC.[xxii],[xxiii] The history of advances in the understanding of the toxic effects of lead over the past thirty years is an outstanding example of how knowledge learned from research can impact in public health. Measures that have had the greatest impact on reducing exposure to lead have been reduction of lead from petrol, elimination of lead solder from canned food, removal of lead from paint, and abatement of housing containing degrading lead-based paint.[xxiv],[xxv] Those countries where these initiatives have been implemented have seen exposures and body burdens of lead decrease.[i] In order to continue to sustain national and international efforts to manage the health risks of lead to children, a lead risk management approach should be taken to: Consult and communicate
Identify the lead risk
Assess the lead risk
Control the lead risk
It remains generally acknowledged that there is no safe level of exposure to lead. Therefore, the lower the level, the better it will be for everyone. References [1] US EPA. Air Quality Criteria for Lead, Vols I to IV. US Environmental Protection Agency, Washington, 1986. [1] ATSDR. Toxicological profile for Lead. Agency for Toxic Substances and Disease Registry, Washington, 1992. [1] ATSDR. Toxicological Profile for Lead. Agency for Toxic Substances and Disease Registry, Washington, August 2007. [1] Gibson, J.L. A plea for painted railings and painted walls of rooms as the source of lead poisoning amongst Queensland children. Australasian Medical Gazette 23: 149-153, 1904. [1] Turner, A.J. On lead poisoning in childhood. British Medical Journal 1: 895–857, 1909. [1] Murozumi, M., Chow, T.J., Patterson, C.C. Chemical concentration of pollutant lead aerosols, terrestrial dusts and sea salts in Greenland and Antarctic snow data. Geochimica et Cosmochimca Acta 33: 1247-1294, 1969. [1] Ericson, J.E., Shirahata, H., Patterson, C.C. Skeletal concentrations of lead in ancient Peruvians. New England Journal of Medicine 300: 946-951, 1979. [1] Pirkle, J.L., Brody, D.J., Gunter, E.W., Kramer, R.A., Paschal, D.C. The decline in blood lead levels in the US. Journal of the American Medical Association 272: 284-291, 1994. [1] Cook, D.E., Gale, S.J. The curious case of the date of introduction of leaded fuel to Australia: Implications for the history of Southern Hemisphere lead pollution. Atmospheric Environment 39: 2553-2557, 2005. [1] CDC. Preventing Lead Poisoning in Young Children. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services, Atlanta, 1991. [i] US EPA. Air Quality Criteria for Lead, Vols I to IV. US Environmental Protection Agency, Washington, 1986. [ii] ATSDR. Toxicological profile for Lead. Agency for Toxic Substances and Disease Registry, Washington, 1992. [iii] ATSDR. Toxicological Profile for Lead. Agency for Toxic Substances and Disease Registry, Washington , August 2007. [iv] Gibson, J.L. A plea for painted railings and painted walls of rooms as the source of lead poisoning amongst Queensland children. Australasian Medical Gazette 23: 149-153, 1904. [v] Turner, A.J. On lead poisoning in childhood. British Medical Journal 1: 895–857, 1909. [vi] Murozumi, M., Chow, T.J., Patterson, C.C. Chemical concentration of pollutant lead aerosols, terrestrial dusts and sea salts in Greenland and Antarctic snow data. Geochimica et Cosmochimca Acta 33: 1247-1294, 1969. [vii] Ericson, J.E., Shirahata, H., Patterson, C.C. Skeletal concentrations of lead in ancient Peruvians. New England Journal of Medicine 300: 946-951, 1979. [viii] Pirkle, J.L., Brody, D.J., Gunter, E.W., Kramer, R.A., Paschal, D.C. The decline in blood lead levels in the US. Journal of the American Medical Association 272: 284-291, 1994. [ix] Cook, D.E., Gale, S.J. The curious case of the date of introduction of leaded fuel to Australia: Implications for the history of Southern Hemisphere lead pollution. Atmospheric Environment 39: 2553-2557, 2005. [x] CDC. Preventing Lead Poisoning in Young Children. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services, Atlanta , 1991. [xi] Bellinger, D.C., Bellinger, A.M. Childhood lead poisoning: the torturous path from science to policy. Journal of Clinical Investigation 116: 853-857, 2006. [xii] NY DoH. Eliminating childhood lead poisoning in New York State by 2010. New York Department of Health. At: http://www.health.ny.gov/environmental/lead/exposure/childhood/finalplanhist.htm [xiii] Needleman, H.L., Gunnoe, C., Leviton, A., Reed, R., Peresie, H., Maher, C., Barrett, P. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. New England Journal of Medicine 300: 689-693, 1979. [xiv] Edwards-Bert, P., Bentley, K., Callan, P., Baghurst, P., editors. Proceedings of the International Meeting on Non-occupational Exposure to Lead, Melbourne , 5-9 October 1992. SAHC, Melbourne , Australia. [xv] CDC. Managing Elevated Blood Lead Levels Among Young Children: Recommendations from the Advisory Committee on Childhood Lead Poisoning Prevention. Nutritional Interventions. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services, Atlanta , 2002. [xvi] NHMRC. Blood Lead Levels for Australians. National Health and Medical Research Council, Canberra , 2009. [xvii] ACCLPP. Low level Lead Exposure Harms Children: A Renewed Call for Primary Prevention. Report of the CDC Advisory Committee on Childhood Lead Poisoning Prevention, Atlanta , January 2012. [xviii] Kosnett, M.J., Wedeen, R.P., Rotherberg, S.J., Hipkins, K.L., Materna, B.L., Schwartz, B.S., Hu, H., Woolf, A. Recommendations for medical management of adult lead exposure. Environmental Health Perspectives 115: 463-471, 2007. [xix] Lustberg, M., Silbergeld, E. Blood lead levels and mortality. Annals of Internal Medicine 162: 2443-2449, 2002. [xx] Wilhelm, M., Heinzow, B., Angerer, J., Schulz, C. Reassessment of critical lead effects by the German Human Biomonitoring Commission results in suspension of the human biomonitoring values (HBM I and HBM II) for lead in blood of children and adults. International Journal of Hygiene and Environmental Health 213: 265-269, 2010. [xxi] Wilhelm, M., Heinzow, B., Angerer, J., Schulz, C. Reassessment of critical lead effects by the German Human Biomonitoring Commission results in suspension of the human biomonitoring values (HBM I and HBM II) for lead in blood of children and adults. International Journal of Hygiene and Environmental Health 213: 265-269, 2010. [xxii] NTP Monograph on Health Effects of Low-level Lead (June 2012) http://ntp.niehs.nih.gov/?objectid=4F04B8EA-B187-9EF2-9F9413C68E76458E
[xxiii] WHO. Childhood Lead Poisoning. World Health Organisation, Geneva , 2010, at: http://www.who.int/ceh/publications/childhoodpoisoning/en/index.html [xxiv] Chisholm, J.J.Jnr. The road to primary prevention of lead toxicity in children. Pediatrics 107: 581-583, 2001. [xxv] Goyer, R.A. Results of lead research: Prenatal exposure and neurological consequences. Environmental Health Perspectives 104: 1050-1054, 1996. |
|||||||
|
About
Us |
bell
system lead poisoning |
Contact Us
| Council
LEAD Project | egroups | Library
- Fact Sheets | Home
Page | Media Releases |
||||||||
|
Last
Updated 06 June 2014
Copyright © The LEAD Group Inc. 1991- 2014 PO Box 161 Summer Hill NSW 2130 Australia Phone: +61 2 9716 0014 |
||||||||